The evolution of endovascular aortic repair has fundamentally changed how thoracoabdominal aortic aneurysms (TAAAs) are approached. What was once considered the exclusive domain of open surgery can now, in selected patients, be treated through entirely endovascular techniques with increasingly sophisticated device platforms.
Among these, Fenestrated EVAR (FEVAR) and Branched EVAR (BEVAR) have emerged as the two principal strategies for preserving visceral perfusion during complex aortic reconstruction. Although often discussed together—and sometimes interchangeably—they are conceptually and technically distinct approaches, each with unique advantages, limitations, and anatomical implications.
Understanding these differences is essential not only for device selection, but also for procedural planning, durability, and long-term management.
The Fundamental Concept
At their core, both FEVAR and BEVAR are designed to solve the same problem: how to achieve an adequate proximal seal while maintaining perfusion to critical branch vessels such as the celiac artery, SMA, and renal arteries.
The distinction lies in how those vessels are incorporated into the graft design.
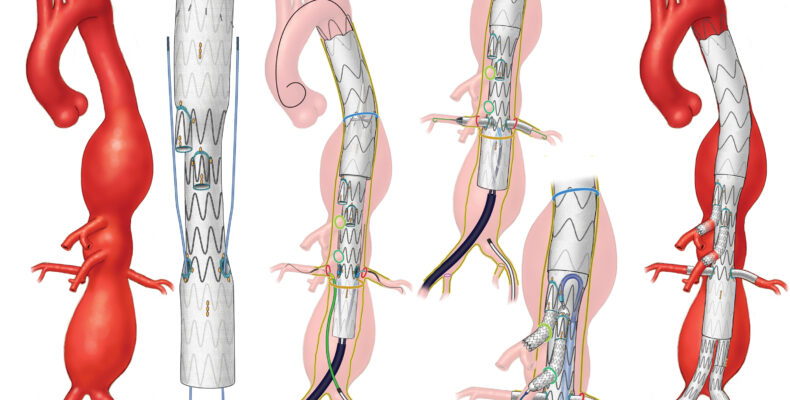
In FEVAR, the graft contains precisely aligned openings—or fenestrations—within the fabric itself. These fenestrations are positioned to correspond directly with the target vessels and are typically bridged with balloon-expandable covered stents.
In BEVAR, the graft contains directional side branches that extend outward from the main body, creating a dedicated conduit between the aortic lumen and the visceral vessels via bridging stents.
While both strategies can achieve excellent outcomes in experienced hands, the anatomical philosophy behind each approach is fundamentally different.

Fenestrated EVAR: Precision Through Apposition
Fenestrated systems rely heavily on precise graft-vessel alignment. The success of the repair depends on the ability to position the fenestrations accurately against the target vessel ostia while maintaining adequate proximal sealing and rotational orientation.
This makes FEVAR particularly attractive in:
- Juxtarenal and pararenal aneurysms
- Short-segment thoracoabdominal pathology
- Patients with relatively narrow aortic lumens
- Cases where visceral vessel takeoff angles remain favorable
The lower profile of fenestrated systems can also be advantageous in patients with restricted access anatomy.
However, FEVAR becomes progressively more challenging as aneurysm extent increases. Large aneurysmal sacs create greater separation between the graft and the native vessel ostia, reducing stability and increasing the difficulty of maintaining durable bridging geometry.
In these settings, the limitations of fenestrations become more apparent.
Branched EVAR: Stability in Complex Anatomy
Branched systems were developed largely in response to the challenges encountered in extensive thoracoabdominal disease.
Unlike fenestrations, directional branches create a physical extension from the graft into the aneurysm sac, allowing the bridging stent to traverse a more stable and controlled path toward the target vessel. This becomes particularly advantageous in:
- Crawford type I–III thoracoabdominal aneurysms
- Large aneurysm diameters
- Wide aortic lumens
- Significant graft-vessel separation
- Complex visceral angulation
The directional branch effectively reduces the unsupported segment of the bridging stent, improving mechanical stability and reducing susceptibility to displacement or kinking.
From a hemodynamic standpoint, branches also tend to create more favorable flow geometry in larger sacs where fenestrations may struggle.
The tradeoff, however, is increased procedural complexity. Branched repairs often require:
- Upper extremity access
- Longer procedural times
- More extensive catheter manipulation
- Larger device profiles
- Greater fluoroscopic burden
As a result, they demand a highly experienced multidisciplinary team and meticulous procedural planning.
Bridging Stents: The True Functional Component
One of the most important concepts in modern TAAA repair is that the durability of the reconstruction often depends less on the main graft and more on the bridging stents.
Whether fenestrated or branched, these bridging components represent the dynamic interface between fixed graft architecture and mobile visceral vessels. They are subjected to:
- Respiratory motion
- Cardiac pulsatility
- Aortic remodeling
- Longitudinal and torsional forces
For this reason, bridging strategy is critical.
Balloon-expandable covered stents provide precision and radial force, particularly useful in fenestrated repairs. Self-expanding systems may offer greater flexibility and conformability in branched configurations or highly mobile anatomy.
The ideal choice is rarely universal and should be individualized based on anatomy and device interaction.
Access Strategy and Procedural Philosophy
FEVAR procedures are often more dependent on precise deployment mechanics and rotational control during initial graft positioning. Small errors in orientation can significantly complicate cannulation.
BEVAR procedures, in contrast, frequently shift complexity downstream into branch catheterization and bridging.
This distinction influences procedural philosophy:
- FEVAR rewards precision during deployment
- BEVAR rewards strategy during branch incorporation
Understanding where complexity resides is essential for planning operative flow, imaging strategy, and bailout options.
Durability and Aortic Remodeling
Long-term durability remains one of the central questions in complex endovascular aortic repair.
Fenestrated repairs generally perform extremely well in anatomies where graft-vessel apposition remains stable over time. However, progressive aneurysmal degeneration may alter branch geometry and increase stress on bridging stents.
Branched systems may offer greater tolerance to future aortic remodeling due to their increased spatial flexibility within larger aneurysm sacs.
That said, neither approach eliminates the underlying degenerative process of aortic disease. Patients remain lifelong vascular patients, requiring structured surveillance and secondary intervention planning.
The Future: Hybridization of Concepts
The distinction between fenestrated and branched repair is becoming increasingly blurred. Modern devices increasingly incorporate hybrid designs, combining fenestrations, branches, scallops, and inner branch technologies within the same platform.
At the same time, off-the-shelf systems are evolving rapidly, aiming to reduce manufacturing delays while expanding anatomical applicability.
The future of TAAA repair will likely not belong exclusively to one concept over the other, but rather to platforms capable of adapting intelligently to patient-specific anatomy.
Closing Perspective
Fenestrated and branched EVAR are not competing technologies so much as complementary strategies within the broader evolution of endovascular aortic therapy.
Each approach reflects a different solution to the same anatomical challenge. The decision between them should not be driven by operator preference alone, but by a careful understanding of aneurysm morphology, branch geometry, access considerations, and long-term durability.
As device technology continues to evolve, the most important determinant of success remains unchanged: thoughtful planning, disciplined execution, and a deep respect for the complexity of aortic disease itself.